

As you’ll have gathered from my previous article the National Gender Service (NGS) and the authors of its Model of Care (MoC) Prof. Donal O’Shea and Dr. Paul Moran not only believe that their MoC is better than WPATH but that WPATH v7 SOC is unsafe. In this, my final article for Trans Awareness Week, I’m going to dig into why they say that’s the case.
The previous article already covered the incorrect claim that WPATH v7 SOC’s informed consent section does not require a mental health assessment. In fact the third paragraph of that section on page 34 discusses the importance of just that, which leads me to question whether the author of NGS analysis of WPATH had read the parts of the WPATH v7 SoC that they were criticising.
The main document I’m going to be analysing here is called “Gender Clinic Operational Model of Care September 2018”, which is presumably part of what Dr. Moran presented to the steering group that established the NGS on 8 September 2018 before the MoC that he and Prof. O’Shea wrote was approved. As the title is a mouthful, I’m going to refer to this document as GCOMoC which is slightly less of a mouthful.
What is a Gender Clinic?
A significant portion of GCOMoC is dedicated to explaining why Gender Clinics are safer than WPATH:

However we quickly run into a problem as this document doesn’t at any point define what a Gender Clinic is, let alone one that is useful for comparing models of care. My understanding of the term is medical clinic whose primary purpose is to provide transgender-related healthcare which should include at a minimum a way to access HRT and surgery. You can start to see the problem here, in that there are such clinics around the world that operate all sorts of models of care; from old-school heavy gatekeeping that presumes that if you’re wearing jeans you can’t be a trans woman, to full-on informed consent where as long as you understand the risks and benefits of HRT they will prescribe.
We do get a hint of what is actually meant from the statement sent to the CEO of TENI on 9 October 2018 following the establishment of the NGS and it’s MoC:

So by Gender Clinic, what it seems to mean is the sort of Gender Clinics that operated in England at the time. Supporting this, GCOMoC also mentions a 2015 NHS report:

The report is titled Operational research report following visits and analysis of Gender Identity Clinics in England and weighs in at 46 pages.
But there’s one tiny problem: The 6 English gender clinics it looks at are all different:

GCOMoC admits this when it attempts to benchmark against the English clinics:
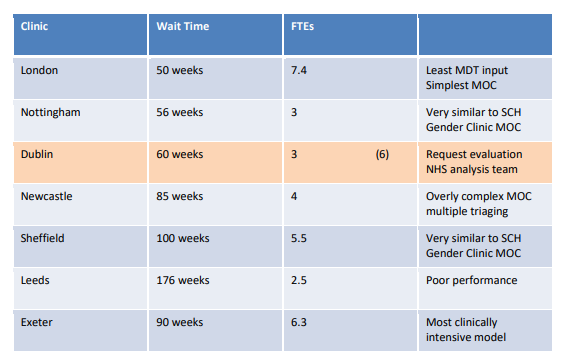
Only two of the clinics are considered “very similar” to what is proposed for the NGS MoC, so the claim that the NGS’s MoC is “in line with the model in the NHS” is starting to look kinda dubious as there is nothing which could be described as “the” model. Oddly some of the notes here are not in line with what is actually written in the NHS report.
For example it is actually Newcastle with its “Overly complex MoC multiple triaging” whose pathway appears closest to the NGS MoC considering the only difference is a multidisciplinary team (MDT) review of the referral before proceeding to the same essential assessment process the NGS MoC has.
Nottingham despite the claim that it is “Very similar to SCH Gender Clinic MOC” is actually quite different, as it lacks any MDT meetings and adds an extra meeting between two doctors, the patient, and a friend. Sheffield is also fairly different, as it adds a clinician screening and lacks the MDT review between the two diagnostic assessments that the NGS MoC has.
This benchmarking is worth unpacking a little, it seems to be trying to make a link between number of staff (FTEs is Full Time Equivalents), the MoC in use, and the waiting time for an initial appointment, and presumably decrying Leeds’ poor performance on this basis. Firstly the waiting times are substantially more than contained in the NHS report so must have been collected independently by the authors of GCOMoC, presumably some time in 2018. Comparing waiting lists in 2018 to the staffing levels in a 2015 report is not going to be particularly illuminating. In addition, for any sort of apples to apples comparison you’d need to consider whether each clinic is getting their fair share of referrals, how long they’ve been running, and which services each clinic provides. For example not all clinics provide speech therapy. So in all, this benchmarking is at best misleading.
These high waiting times are also interesting, but first a detour into why this NHS report exists:

This report is at its core looking at the gender clinics from a queuing theory standpoint. The report looks for any approaches that some clinics are taking that could be applied to improve waiting lists elsewhere, watches out for potential pitfalls, and projects what is likely to happen to the waiting lists in future. As a piece of work I am thoroughly impressed with this NHS report, it really tingles my it pronoun. To those who have read some of my older articles this will not come as a surprise, as I applied some of the same underlying principles to predict where the NGS waiting list was going and try to understand where the NGS spends its time.
A key point is that the NHS has a 18 week target from first referral to being treated, and the NHS report is quite concerned about what needs to be done to achieve this target. So the fact that the 2018 numbers are all far in excess of 18 weeks should be taken as all of these clinics have severe issues. For a bit more background on this I cannot recommend strongly enough the recent video from Philosophy Tube on this topic. Whether you are trans or a cis ally this is essential watching to understand why trans healthcare is in the poor state it is. The authors of GCOMoC never mention this failing, which makes me wonder how carefully they read the NHS report. A report which mentions this 18 week target no fewer than 15 times.
GCOMoC tells us that this NHS report is full of both qualitative and quantitative operational outcomes:

However as you might have gathered, the NHS report is entirely about quantitative outcomes: How long are the waiting lists and what do we need for staffing to keep it under control. There are no qualitative outcomes as GCOMoC claims, which the NHS report mentions as something that needs fixing in its Overall Conclusions:

Let’s look at the relationship between the English Gender Clinics and WPATH. The NHS report says:

Section 11.3 of the report is a comparison with the WPATH v7 SoC, identifying roles that a Gender Clinic would need to fill, and found that the 6 English Gender Clinics fulfilled those roles. The main differences between the clinics in terms of WPATH was around how psychological support was provided:

Finally I’d like to look back at the top of the section, which has following from GCOMoC:
This makes it seem as though English Gender Clinics and WPATH are very different things. However from reading the NHS report it is clear that the English Gender Clinics follow WPATH v7 SOC as indeed I would expect most gender clinics to. I also question the extraordinary claim that there’s no published research for WPATH services, considering that WPATH SOCs are a consensus based on the experiences of medical professionals working with transgender professionals around the world.
That includes research from the English Gender Clinics. The NHS report happens to mention that Nottingham contributes to leading research, so I looked at the references in WPATH v8 SOC for Nottingham staff as that’s always a good starting point to find well regarded scientific studies. I found 26 papers, of which 14 were published before 2018 when GCOMoC was written. So not only is there plenty of research from WPATH based services, but some of it originates from the very Gender Clinics that GCOMoC praises. If that’s not enough, Appendix D of WPATH v7 SOC provides numerous studies of outcomes following the WPATH SOCs being put in place.
To summarise the NGS claims to be following the NHS Gender Clinic model, because this is safer than WPATH. However it turns out that the NHS report GCOMoC relies on reveals 6 different models none of which exactly match the NGS MoC and all of which follow WPATH. GCOMoC claims that there’s little research of WPATH based services, however a quick search found 14 papers from one of the WPATH-following NGS Gender Clinics which GCOMoC (incorrectly) says follows a very similar MoC to NGS, and all of which would have been available at the time GCOMoC was written.
I find it a worrying sign that, from analysing merely a page and a bit of GCOMoC, that there is a consistent pattern where it appears the authors of GCOMoC haven’t properly read and understood the NHS report which they were basing this part of the document on.
Comorbidity
Content Warning: Discussion of suicide, search forward for “2017 QID MoC” to skip to the next section.
Comorbidity is the medical way of saying you have more than one illness happening in a person at the same time.
Continuing on its argument that Gender Clinics are safer than WPATH, GCOMoC looks at mental illness of trans people:

It does indeed seem true that many mental issues are known to more common among trans people than their cis counterparts, though we’re not sure why.
The argument following that is a bit lacking though:

What are these consequences? I’m afraid they’re not obvious to me. Continuing on however we can start to figure out what is probably meant by this vague statement.
GCOMoC goes on to talk about a 30 year follow-up study from Sweden after SRS, summarising it as:

There’s a number missing there, which is 19.1 per the study. It is interesting to note that this study is often misrepresented, as the study’s author says:

GCOMoC goes on to quote the conclusion of the study, and then in the next sentence makes a big leap:

So a single study suggests that after SRS, usually the final stage of medical transition for those who choose to have it, some ongoing mental health support might be an idea to help with the increased suicidality.
GCOMoC jumps from this study’s conclusion into saying that a multidisciplinary team plus psychiatry is essential at the very start of the assessment process, which is well before SRS would be considered. Further it proposes that one way you can do WPATH should be avoided, however once again this would only affect the very beginning of the typical pathway that would lead to SRS so this doesn’t follow from what the study found.
There’s other odd things about this leap. As discussed above, the NHS Gender Clinics which GCOMoC holds up as being safer than WPATH have a variety of models of care, and only two of them require a multidisciplinary team as part of the assessment for all patients. Similarly one of the Exeter Gender Clinics has no psychiatrists, and Leeds relies primarily on mental health nurses for this role.
If we peek into the NGS MoC it doesn’t have a role for this “embedded MDT and psychiatry” once transition is complete:

So this MDT and psychiatry wouldn’t even be available to someone post-SRS. So not only does a WPATH model network of external referring specialists supposedly not allow for ongoing support, but neither does the NGS MoC and thus the NGS MoC would appear to be unsafe per the arguments of GCOMoC.
The 9 October 2018 statement to TENI has a similar leap:

Here the presumption is that the increased suicide rate is due to some pre-existing mental health problem that could have been caught at the initial assessment. It’s also presuming that only a psychiatrist could catch this, and not say a clinical psychologist. I’ll leave it to the author of the Swedish study to explain why this purely numerical correlation is not likely to be causation:
Once again it would seem that the arguments made by GCOMoC are not backed up by the sources it references, and do not support their argument that a multidisciplinary team with psychiatry is essential for a safe service.
2017 QID MoC
When analysing GCOMoC one must keep in mind that at a political level the question is not NGS MoC vs WPATH, but NGS MoC vs the 2017 QID MoC which was led by Dr. Philp Crowley of the HSE’s Quality Improvement Division (QID) and which is guided by WPATH v7 SOC.
Accordingly it is instructive to compare the two MoCs. It’s easiest to reuse the comparison prepared by Dr. Philip Crowley and Dr. Siobhán NíBhrian prepared in February 2021, as it aligns with my understanding of both MoCs:
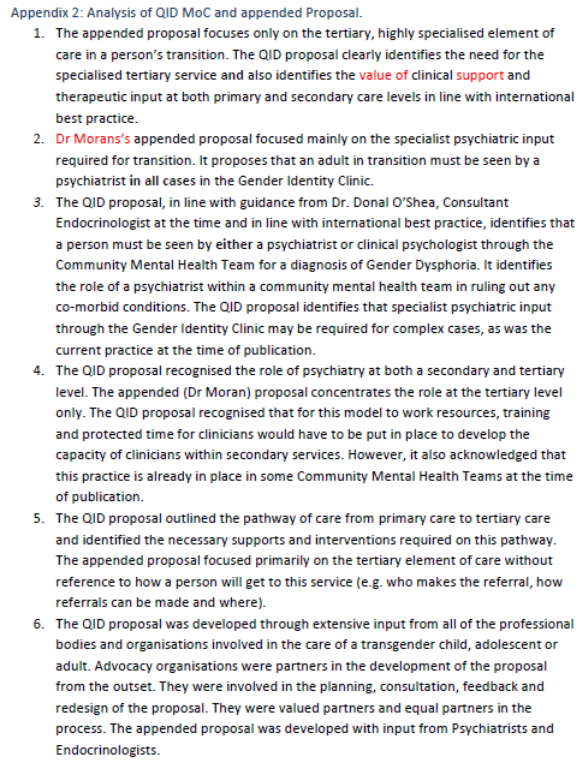
The 2017 QID MoC also proposes making the defacto gender clinic in Loughlinstown into an official National Gender Identity Clinic, and expanding the services it provides, which you’d think the people working there would appreciate. It has other improvements such as adding hair removal, and using the Community Mental Health Teams to provide on-going support – which is along the lines of what the Swedish study in the previous section actually suggested and is thus in the terms of GCOMoC a safe MoC.
The major difference is that the 2017 QID MoC has the diagnosis of gender dysphoria be done by a panel of psychiatrists and clinical psychologists around the country with appropriate gender-related training and including considering comorbid conditions, whereas the NGS MoC consolidates this entirely within psychiatrists in the NGS.
Why the authors of the NGS MoC Dr. Paul Moran and Prof. Donal O’Shea might be so invested in having a psychiatric assessment solely happen in the NGS? The reasoning of GCOMoC which is superficially astute falls apart at the slightest scrutiny, reasoning which when correctly applied indicates that the NGS MoC is unsafe and the 2017 QID MoC safe. I will make one final observation.
At the time the NGS MoC was being approved by the steering group the psychiatrist working in what became the NGS was Dr. Paul Moran.
While Jessica Black (she/it)’s pronouns may sound like shit, a connoisseur of puns would appreciate that they’re a shite typo.
Featured image via Flickr – wp paarz

